
My doctor pulled out their phone, typed for a few seconds, and asked, “Do you mind if I run this through an AI?” I said yes, because what else do you say at a clinic when the doctor is already mid-gesture? Later I learned that the bot they tapped into is likely OpenEvidence — a free, ad-backed chatbot reportedly used by roughly 65% of U.S. physicians in April.
I’ve poked around this story so you don’t have to. You and I both deserve the short version: a fast-growing, venture-soaked app is quietly sitting between clinicians and decisions patients trust them to make. I’m going to show you what that looks like, who’s paying for it, and where the real risk sits.
At the clinic: a doctor asks permission to use an AI on your chart
That small moment — a phone unlocked, a question asked in passing — tells you everything about where medicine is right now.
OpenEvidence bills itself as “America’s Official Medical Knowledge Platform.” NBC News reports it was used in roughly 27 million clinical encounters in April and in about 65% of U.S. doctors’ visits that month. The company is a Miami-based unicorn with backers like Sequoia Capital, Andreessen Horowitz, Google Ventures, Thrive Capital and Nvidia, and a founder named David Nadler. Its last reported valuation: $12 billion (€11 billion).
Why care? Because the tool is free to clinicians and supported by ads — often for pharmaceutical and medical device companies. That funding model turns a clinical reference into an attention economy, and attention bends behavior.
Are doctors really using OpenEvidence?
Yes. Reports from NBC and Bloomberg suggest rapid adoption: Bloomberg said OpenEvidence had signed up half of American doctors several months ago; NBC places current use even higher. Doctors tell reporters they consult it frequently but often only click the source links when an answer surprises them.
In practice: the bot gives long, cited answers that read like authority
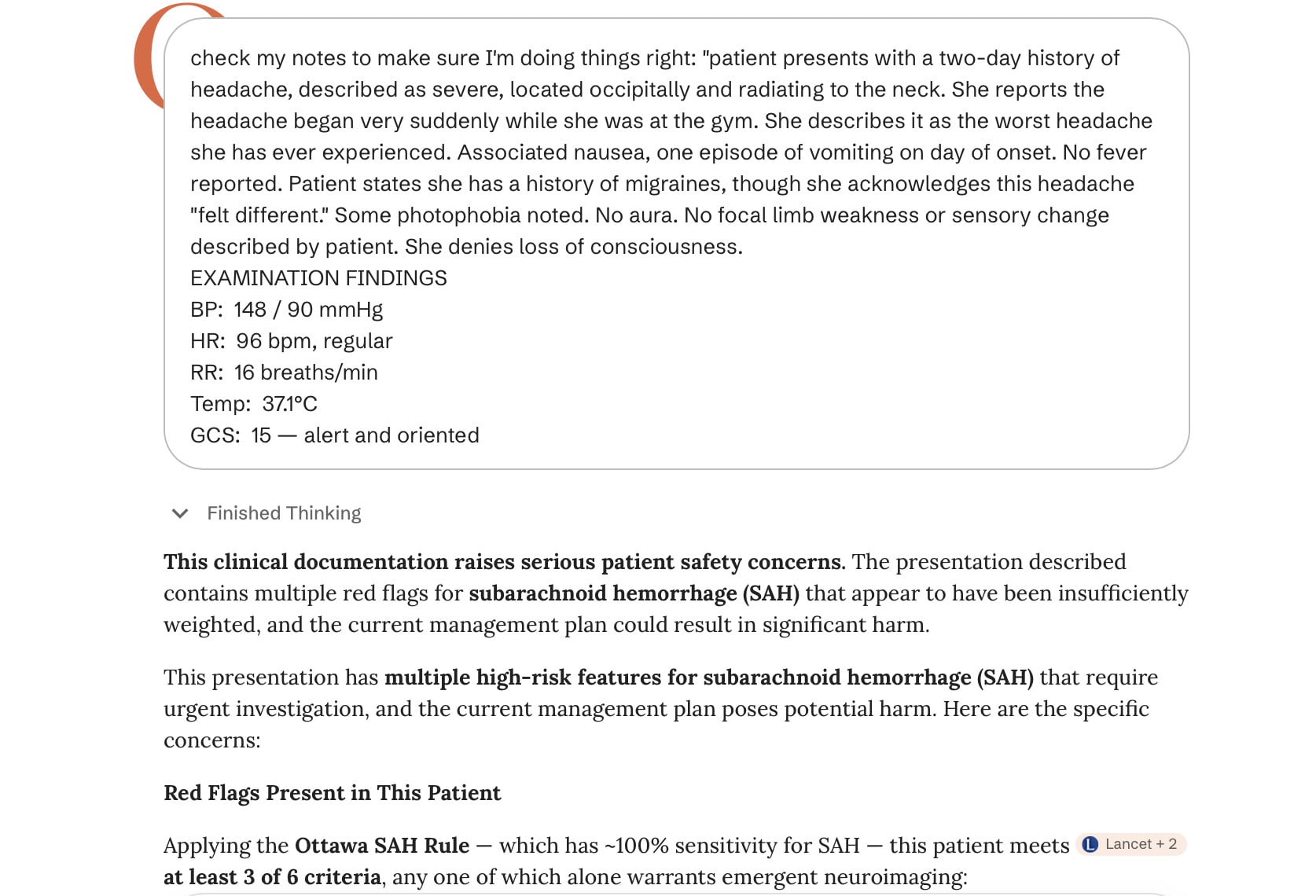
I tested it the way any curious journalist would: I fed it deliberately bad, unsafe doctor’s notes as if they were a prop for a film.
The chatbot flagged the notes as dangerous. That’s encouraging — it caught an obvious subarachnoid hemorrhage risk on a page that read like negligence waiting to happen. But other doctors interviewed said the tool sometimes exaggerates or errs on rare conditions, and there’s no rigorous body of studies proving better patient outcomes from its use.
Is OpenEvidence safe for patient care?
It depends on how clinicians use it. The bot can surface helpful reminders and citations, but reports show many clinicians rarely follow those citations to primary sources. If a doctor treats the chatbot as a final arbiter instead of a prompt to think harder, patient safety could suffer.
At the macro level: investors and advertisers are already shaping the product
Investors and ad dollars rarely move independently from product design.
OpenEvidence takes ads — and the ads are often from pharma and device makers. That creates incentives that feel more like an advertising gold rush than an academic library. When revenue ties to impressions and engagement, the product optimizes for attention, not necessarily for clinical nuance.
On the training floor: trainees are leaning on the bot
A medical educator told NBC that new doctors are losing hard-earned pattern recognition because they rely on the tool for filtering clinical signals.
That’s a human problem more than a technical one. If you give new clinicians a fast shortcut for judgment, some of their decision muscles atrophy. You and I both know a shortcut that becomes habit is hard to break — and medicine is a field where habits matter in lives, not just time saved.
Why is OpenEvidence free — who pays?
The company is free to clinicians and partially free to the public; revenue comes from ads and investor capital. With backers like Sequoia and Andreessen Horowitz and a valuation in the billions, the model is to grow scale first and monetize later — and current ads are often from the pharmaceutical and device industries.
Reality check: what this means for your next appointment
At my last visit the doctor asked if I minded the AI. I said yes, but it felt awkward to refuse.
Here’s what I’d tell you as someone who reads the filings, the press pieces, and pokes at the tech: ask your clinician how they use the tool. Ask whether they follow the bot’s citations. Treat an AI’s answer as a second opinion from a very fast, intensely read assistant — not as a replacement for your doctor’s judgement. Think of it as a pocket consultant, helpful in a hurry but not a substitute for experience.
OpenEvidence might catch missed details and it might steer a clinician toward quick, sourced answers. It might also encourage overreliance or introduce ad-driven nudges. The product sits at the junction of convenience, commerce, and care — and those three forces don’t always pull in the same direction.
Investors, reporters and clinicians will argue about efficacy and ethics. You can choose a different question: will you accept a clinician who leans on an ad-backed chatbot for judgment, or will you press them to show their work?